
Inflammatory Bowel Disease (IBD) may cause a variety of symptoms beyond the bowel. Along with gastrointestinal symptoms, there may be symptoms due to the involvement of joints, skin, eyes, liver and bile ducts, kidneys and bones.
Liver and the involvement of bile ducts can lead to fatty liver, hepatitis, gallstones, and Primary Sclerosing Cholangitis (PSC).
The gallbladder is situated near the largest organ in our body, the liver. The liver makes bile liquid and sends it to gallbladder, where it is stored. When you digest fatty foods, the bile is released from gallbladder. Bile ducts are long, thin, tube-like structures that carry bile to the small intestine. Bile breaks down the fat, which helps in digestion.
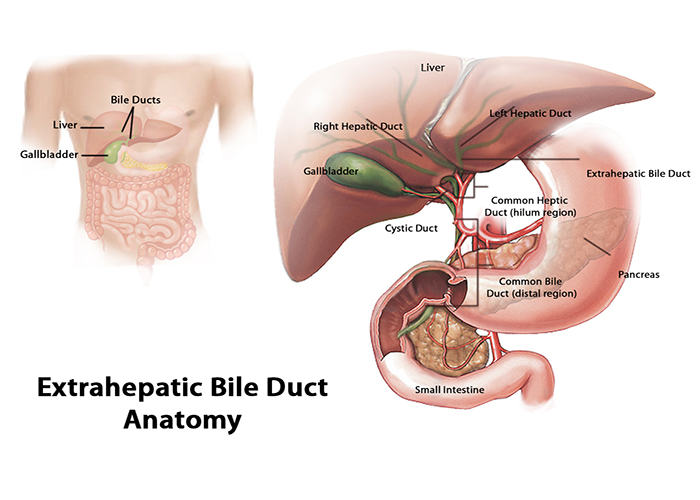
Primary sclerosing cholangitis, a disease of bile ducts, is a rare disorder that affects males twice as often as females. Inflammation, scarring and a narrowing of the ducts occurs, which causes disruption in the normal flow of bile. Buildup of bile in the liver gradually causes serious liver damage.
PSC occurs most often in middle-aged adults. The exact cause of PSC is not known. It is believed to be caused by the immune system’s reaction to an infection or toxin in people with a genetic predisposition to the condition. A higher risk of primary sclerosing cholangitis is seen in people with northern European heritage.
Early signs and symptoms of PSC often include jaundice (yellow eyes and skin), fatigue, itching and abdominal pain. As the disease progresses, people may experience fever, night sweats, chills, weight loss, enlarged liver and spleen.
Most people with PSC have underlying inflammatory bowel disease. The prevalence of IBD in patients with PSC is close to 90%. The prevalence of Ulcerative Colitis is higher than Crohn’s disease. People with concurrent PSC and IBD have an increased risk of colorectal cancer.
It is important to let your doctor know if you have IBD plus unexplained fatigue and itching, in order to rule out the possibility of PSC.
The incidence of PSC among immediate relatives, especially siblings, is higher than would be expected, indicating that genetics plays an important role in the development of PSC. Researchers have discovered 16 different genetic regions associated with this disorder. Several genetic regions associated with PSC are also associated with IBD.
Inflammatory bowel disease often presents at an earlier age in people with PSC, as compared to people with only IBD. When IBD is associated with PSC, it is generally mild or quiescent and often asymptomatic. In rare cases, there may be rectal bleeding.
Given the high prevalence of IBD in patients with PSC, a colonoscopy is generally done by doctors at the time of PSC initial diagnosis, regardless of the presence of IBD symptoms. A colonoscopy is also the screening test for IBD and colorectal cancer.
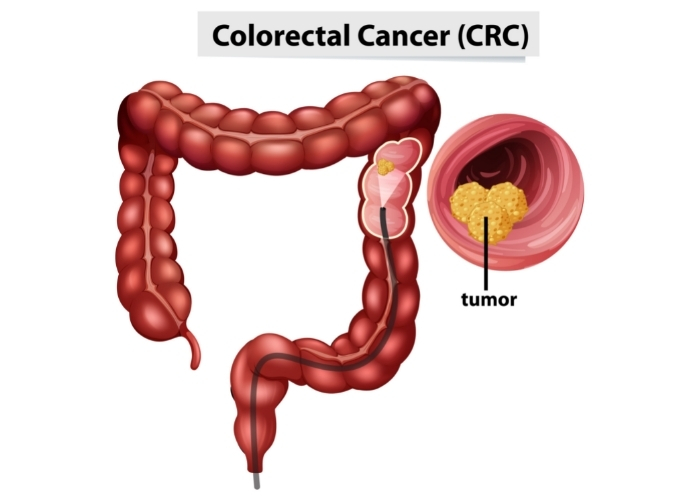
The mechanism by which concomitant PSC increases the risk of colorectal cancer in patients with IBD is unknown. Chronic inflammatory activity may be the driver. Other complications include cirrhosis of the liver, bile infection (Cholangitis), and cancer of the bile duct system (Cholangiocarcinoma).
Unfortunately, there is no treatment for PSC. Stents are usually placed within the bile ducts to keep the bile flowing and to control bile build-up.